
Sometime in 1997 when he was in his early teens, Dr Vinay Kumar learnt that he had to take an injection every day to treat an ailment. For the youngster from a village near Shamli in western Uttar Pradesh, where “an Atlas bicycle was the Mercedes Benz” of the family and buffaloes were beloved members of the household, that meant a new regimen nobody had heard of, or could fathom. The first task of the day was to travel to a compounder in a nearby village—because his place didn’t have a doctor—and get a shot of insulin. “So, sometimes my breakfast was by noon or 1 pm or so...those were the horrible days,” recounts Kumar, co-founder of a startup called PathShodh in Bangalore, whose much-feted product is a handheld biosensing device for measuring key parameters in managing diabetes and related complications. “From that time on, I’ve been on insulin injections.” If he were to actually take a count, it’s probably well over 30,000 shots.
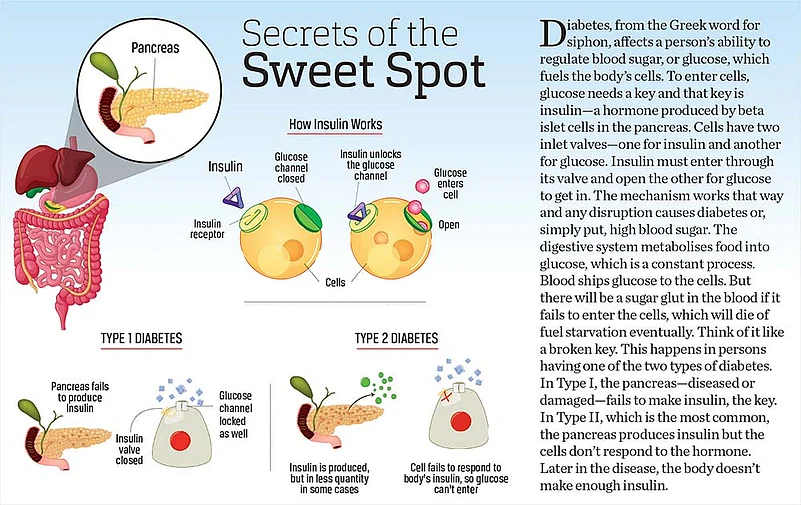
Several times, that hungry wait for a jab turned the see-saw swinging to the other side—dangerously low sugar levels causing blackouts that landed him in an ICU room. On one occasion, Kumar recalls opening his eyes after several comatose hours and the doctor anxiously asking him to remember a number, checking for brain damage. The ever-present tightrope walk between two deadly outcomes is what defines life for those, like Kumar, with juvenile diabetes, or more accurately Type 1 diabetes (see graphic, p.24). But insulin, painful as the injections are, is a blessing. “We survive because of these vials,” he says.




That’s been the story for a hundred years now, ever since 1921 when the long and elusive search for a protein hormone—whose absence caused those runaway glucose levels in the bloodstream—came to an end at the University of Toronto. As fascinating journeys of scientific discoveries go, this too had its share of surprise and chance. Frederick Grant Banting, the discoverer, was after all an orthopaedic surgeon, who succeeded where many others hadn’t, and his breakthrough had come at least three decades after the connection between certain tissues in the pancreas and carbohydrate metabolism had first been guessed at. The gist of that storied event is as follows: Banting came across an article about how a gallstone in a man had blocked the pancreatic duct, causing the enzyme-producing parts of the pancreas to degenerate. Along with his assistant Charles Best, he tried to replicate that effect by tying up the pancreatic ducts in dogs—the digestive enzymes had so far prevented the extraction of the secretion (insulin) produced in another part of the pancreas, so getting rid of them allowed him to extract insulin. It wasn’t long before this life-saving extraction went into commercial production and Banting and John James MacLeod won the Nobel Prize for the discovery. But where one quest ended, another began—one that still continues to this day in the form of newer forms of insulin and delivery mechanisms.
Indeed, it’s been a long road—with several milestones dotting the landscape in terms of treatment—from those early days, all painstakingly built on volumes of research, clinical expertise and sheer experience. But look at the disease itself over the course of these hundred years. The prevalence of diabetes has only been growing—here, we are talking about the most common form of the ailment that afflicts millions across the globe and which has more to do with lifestyles and diet, namely Type 2 diabetes. Nearly half-a-billion people worldwide, it is estimated, live with diabetes, the numbers growing almost five-fold in the past 40 years. In India, with an estimated 77 million people with diabetes, roughly 6 million are on insulin therapy. “There is a gap in awareness, in diagnosis and detection, in treatment initiation and in insulin initiation,” says Vikrant Shrotriya, managing director of Novo Nordisk India. The general thumb rule, he says, is that 30 per cent of diabetics may require insulin.
During the Covid-19 pandemic, says Shrotriya, there has been increased adoption of insulin overall, given the high glycaemic levels associated with Covid treatments. “It has brought a lot of awareness among doctors as well as among the patients in terms of acceptance of treatment,” he adds.
Yet, several studies point out that insulin availability, and affordability, is still a problem in many low- and middle-income countries, India included. Nearly 95 per cent of insulin supply globally comes from three big firms—Eli Lilly, Novo Nordisk and Sanofi. The market for insulin in India is roughly Rs 3,500 crore to Rs 4,000 crore annually.
But back to the insulin story itself. The first insulin was derived from animal sources, hence the quest for higher purity levels marked those early years and the efforts paid off. But things changed dramatically by the 1980s when genetically engineered human insulin hit the market—recombinant technology, by which a human gene was introduced into bacteria to produce insulin, weaned it off animal sources and also lowered costs in mass production. The era of human insulin, so to speak, began.
Even then, another goal still held out—being able to mimic the way the normal pancreas controls insulin secretion in the body by keeping a close watch on glucose levels and releasing just enough to maintain that essential balance. It’s been the dominant theme of insulin research for decades. Think of the vast assortment of insulin delivery devices that have rolled out since: insulin pens and pumps (which went from backpacks to palm size) were invented to replace injections (briefly, there was even an insulin inhaler). In the late 1990s came the insulin analogues—that is, analogous to the basal and bolus cycles, or the lows and highs of insulin requirement during mealtimes and in between.

“The body always maintains what is known as the basal level of insulin,” explains Vinay Kumar, who has been using an insulin pump in recent years. Those too have their own challenges, he says. In a normal pancreas, there’s a knock on its door requesting a release of insulin whenever the sugar level increases in the body. A range of short-acting and long-acting insulin analogues are available now. “Insulin of today is different from the insulin of yesterday,” says Shrotriya. The new generation of insulin, he says, last up to 42 hours, while also reducing the fear of hypoglycaemia, i.e. very low sugar levels. “With the new generation insulin, doctors can target better control,” he says, “When you give insulin in optimum quantity, there is a risk somebody can go into less sugar, but these are insulin which reduce that fear.”
For Type 2 diabetes, the search for non-insulin treatments too is going on. For example, it had been known for decades that a gut hormone called Glucagon-like-Peptide (GLP-1) was involved in stimulating the pancreas to produce more insulin. Now, the first tablets in that category are entering the market (injections came earlier). “Evidence suggests that in India, like many other low- and middle-income countries, access to insulin is constrained due to its limited physical availability and unaffordable prices,” says Abhishek Sharma, a researcher at the department of global health in Boston University School of Public Health. Human insulin is among the essential medicines list of the WHO—its target is that these medicines be made available in at least 80 per cent of health facilities. In a 2016 paper, Sharma noted that only 44.4 per cent of the private pharmacies in Delhi stocked human insulin products and the availability of analogue insulin products was even lower. A later survey in Bangalore, he says, found that the private-sector insulin availability was closer to the 80 per cent, though public-sector availability was lower. Typically, analogue insulin is more expensive than human insulin, while both human and analogue cost more in the cartridge and pen form compared to vials. In the Bangalore private retail sector, prices of human insulin cartridges and pens were 2.5 and 3.6 times higher than the price of vials (Rs 323.5) respectively, his study had found.
As is the case globally, these studies suggested that the retail market is dominated by the big three. “This is despite the fact that same insulin products—in terms of type and delivery device—manufactured by Indian companies (Biocon, Wockhardt) were often sold at a lower price compared to those manufactured by foreign MNCs,” says Sharma. To improve insulin availability and affordability, the government should streamline insulin procurement and supply chains at different levels and develop evidence-based guidelines that prioritise the use of less-expensive, quality-assured human insulin, suggests Sharma. “It would entail a raft of other measures—like mandating biosimilar prescribing and educating physicians to pursue evidence-based prescribing,” he says. “As more Indian companies produce biosimilars, brand substitution policies are needed to be able to benefit from market competition.”
ALSO READ: Diabetes Is A Bad Actor: Dr Shriram Nene
Kumar of PathShodh frames that scenario from the patient’s view. “I think it is more or less accessible now. But which type of insulin is accessible, this is the question,” he says. “For young children with Type 1 diabetes, that’s a crucial determinant of quality of life.” Kumar recounts how he learnt to inject himself—it wasn’t until a few weeks of daily injections that the compounder told him that his shots were going to be a lifelong affair. “I cried a lot after returning home and I cried for the next few days,” says Kumar. “At that time, I learnt to inject insulin myself.” For the vast majority of people suffering from either form of diabetes, there’s hope that technological breakthroughs will change things, perhaps even radically. Take the quest for oral insulin, for instance. A challenge as old as the discovery of insulin. “A lot of research is going on. I’m hopeful that maybe this decade some breakthroughs will come,” says Kumar.
***
1921 Dr Frederick G. Banting starts experiments at the University of Toronto to extract secretions from the Islets of Langerhans, clusters of cells located in the pancreas—the novel idea was to ligate (tie up) the pancreatic duct (the experiments were done on dogs) so that the parts producing digestive enzymes will degenerate but leave the Islets intact (insulin takes it name from the Latin word for island, ‘insula’)
1922 Fourteen-year-old Leonard Thompson, a juvenile diabetic, becomes the first person to have been treated with an insulin injection. The first dose apparently caused an allergic reaction because of the impurities, but subsequent doses, after refinement, were successful—Thompson eventually died of pneumonia in 1935.
1923 American firm Eli Lilly begins commercial supply of insulin. In Denmark, Nordisk Insulinlaboratorium also starts production.
Mid-1960s Insulin becomes the first protein to be chemically synthesised
1978 Human insulin is produced by genetic engineering—via E.Coli bacterium
1985 Novo (later to become Novo Nordisk) launches Novopen, the first insulin pen
2000 Insulin glargine, the first long-acting basal insulin analogue by Aventis (later merged with Sanofi), gets approval
(This appeared in the print edition as "Bitter Sweet")





















