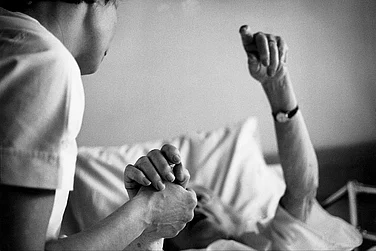
Sitting in her small house in Kotana village in Baghpat district of western Uttar Pradesh, 25-year-old Ruby tells the local anganwadi worker yet again that she won’t vaccinate her 16-day-old son as her husband has refused permission. This is the third visit by Beena Devi, the anganwadi worker of the area, to Ruby’s home in the Muslim basti of the village. Under the government’s Universal Immunisation Programme (UIP), she is required to make calls at and inquire about all newborn children and keep track of the immunisation schedule of each child. It is a task that has proven to be almost unachievable in most parts of state.
The universal immunisation programme under the government of India aims to immunise all newborns and children up to the age of 16. According to World Bank data, the under-5 child mortality rate in India is 48 children per 1,000 births. Vaccination is the most cost-effective intervention available to reduce deaths due to preventable diseases.
In India, over 85 per cent of all immunisation is done free of cost under the government programme. This is done in the villages with the help of Accredited Social Health Activists (ASHAs) and anganwadi workers along with primary health centres (PHCs) and community health centres (CHCs).




Ruby’s case is just one of many similar examples. Ruby had gone to the local anganwadi and taken the two vaccines pregnant women are supposed to take under the programme, but, after her son was born, her husband refused to let the newborn be vaccinated. “That was because several WhatsApp messages have been circulating that say the government is trying to make Muslim children sterile through vaccination,” says Ruby. According to Beena Devi, one of the two resident anganwadi workers in Kotana village, the rumours were possible only because there is lack of awareness about the immunisation programme.
Asara, a village nearly 30 km from Kotana, also faces a similar situation. A substantial number of Muslims live in Asara, which has two ASHA workers along with four Community Mobilisation Coordinators (CMC). While the CMCs help in spreading awareness about immunisation, only the ASHA workers have been trained to administer the vaccines to children and pregnant women. Health workers reveal that both Asara and Kotana have seen cases of polio, pneumonia and measles in the past two years—diseases for which vaccination is mandatory under the government programme.

The Mangadpur anganwadi has been locked for the past two months
Lack of awareness is only one of several issues hampering the UIP in Uttar Pradesh. According to World Health Organisation report, UP is one of the worst states for the implementation of the UIP, with only 57.4 per cent of the children immunised. Visits to some of the villages reveal lack of human resources and inadequate equipment and infrastructure for immunisation, besides little push to spread awareness.
Both Kotana and Asara, villages with population of 12,000 and 36,000 respectively, have only two anganwadi workers. They have to make home visits every day to ensure the families avail of their services in all matters related to healthcare. While Asara has a few trained CMC workers, Kotana has no resident ASHA worker. Instead, the ASHA worker visits Kotana on Wednesday and Saturday when vaccines are administered in the anganwadis under government rules. “We are short-staffed and, in special cases such as that Ruby’s, we often need people with more knowledge and medical experience to talk to the family,” says Beena Devi, who also points out that while there are seven anganwadi centres in the district, most remain closed even on the immunisation days. Moreover, most anganwadis are ill-equipped to handle the immunisation programme—another deterrent to making young mothers understand the need to get their children vaccinated.
Asreen is yet to have her one-month-old baby vaccinated. She had delivered the child at her home in Asara and not in a hospital where the three initial vaccines—BCG, polio and Hep-B—are administered at birth. ASHA worker Sarla, who oversees the work in the region, says the delay is because the doctor did not want to open a new vial of BCG vaccine for just one child and was waiting for a few more children who need the vaccination. “Each vial of BCG contains 10 doses and if all 10 are not used around the same time, they go waste,” says Sarla. “So when there is only one child, the parents are usually asked to come back on the next immunisation day, hoping more children might be brought for vaccination then.” This often results in children not getting vaccinated at the right time.
In Mangadpur village, a few kilometres from Kotana, one anganwadi serves a population of 350 people, but has been locked up for the past two months. Manoj Kumar, the head administrator of the local primary school, reveals that in the past one year, the anganwadi has been opened for immunisation only a handful of times. “The village does have an ASHA worker who keeps track of newborn children, but we have seen no immunisation drives in the past few years,” says Manoj. A quick visit to the ASHA worker’s house reveals that as she has to tend to her fields on most days, she is unavailable for consultations and advice to parents.
Despite the high population, Asara does not have a PHC. The village does have a Unani clinic under the government’s AYUSH programme, but it is dilapidated and does not stock any allopathic medicine. Dr Farhan, the only doctor available at the clinic, says he doesn’t get too many patients, except those requiring counselling on vaccines. “Sometimes if mothers are unwilling to get their children vaccinated, the ASHA workers bring them to us for counselling,” Farhan tells Outlook.
The closest hospital for these villages is the CHC at Baraut, a small city in Baghpat district that is nearly 30 km from Asara and 20 km from Kotana. Around 300 babies are born on an average every month at the CHC, which also serves as the primary cold storage for vaccines for more than 180 villages in the vicinity. “There are four PHCs too in Baraut, but most villagers prefer the CHC since the quality of care and resources are relatively much better there,” says Sachin Malik, the UIP manager at the hospital, showing the four freezers meant for vaccines.
The situation is no different in Gorakhpur district of eastern UP. The BRD Medical College and Hospital, the biggest hospital in the district, serves thousands of patients every day. It is also the district warehouse for vaccines. Gorakhpur is among 11 districts in the country where a large number of cases of Japanese Encephalitis (JE) have been reported. The high incidence of the disease, which causes fever and affects the child’s brain, has forced the government to introduce a vaccine for JE under the UIP in Gorakhpur, but lack of awareness about the UIP and the availability of free vaccines under it have hindered the outcome.
While the hospital administration claims that the vaccination programme covers almost 95 per cent of the population, people from surrounding villages have a different story to tell. Uma of Misrauli village says that while she was lucky enough to get her child vaccinated in the hospital, her village and the smaller villages around are not well covered under the programme. “More often than not, even when ASHA workers come to the village for vaccination, we are not informed and are unable to get our children vaccinated here,” she says.
The BRD Medical College reported around four cases of measles and several cases of polio in the past two years. What sets Gorakhpur apart from other districts is the rise in the number of Acute Encephalitis Syndrome (AES). The hospital sees around 2,000 cases of encephalitis every year. JE is just one of the types of AES, which is used as an umbrella term for all kinds of encephalitis. According to Dr Mahima Mittal, head of paediatrics at the medical college, only around 10 per cent of all AES cases are found to be JE. “The number of JE cases has gone down in the past few years. Now only 10 per cent of all AES cases are reported to be JE. The number has reduced sharply from 50 per cent in the past five years,” says Dr Mittal.
According to government data, Gorakhpur saw 2,208 cases of AES in 2014, 1,760 cases in 2015 and 1,965 cases in 2016, out of which only 173 were JE. Even though only a small percentage of children suffering from AES have JE, the government is not taking any measures to provide immunisation for the other kinds of encephalitis. Dr K.P. Kushwaha, former head of paediatrics at the BRD Medical College, rues the lack of governmental will to promote research for developing a vaccine that might encompass more kinds of AES. “Much research has been done on acute encephalitis syndrome, which suggests the origins of the disease and clear indications on how to cure it. Yet most government organisations, including the ICMR and other research labs, have ignored such evidence and continue to treat only a small part of AES by focusing only on JE,” he says.
While the government’s mechanism for immunisation might be in place at the district levels, for it to reach the village under the ‘immunisation for all’ promise, the government needs to go the extra mile. This does not only include providing more resources in the villages, but also creating more awareness and convincing the people about the benefits of vaccines. Else lapses in the UIP will nullify the purpose, money and the time spent to make it fruitful.
By Arushi Bedi in Baghpat & Gorakhpur