"I have been waiting for over a year in Canada to have an abdominoplasty, liposuction, and breast lift and reduction performed. I am 55 years old and really want to get on with these surgeries as soon as possible."
"We have no health insurance. My wife suffers constantly with her back pain. We cannot even begin to think about treatment here in the US because of the extremely high cost. After seeing your operations on 60 Minutes, we both have new hope. Please contact us."
"Can you tell me what I would have to do to get a referral to your fine hospital and what it might cost to fix my problem?. I have never been outside of the usa...I await your reply with fingers crossed (for good luck)."
Shortly after it was featured in the American TV programme 60 Minutes, e-mails began hitting the inbox of Delhi's Indraprastha Apollo Hospital, seconds apart from each other. From Illinois, Florida, Washington, Texas, New Mexico, California, Oregon, Oklahoma, Tennessee, Virginia, from British Columbia and Alberta, Canada. Curious, hopeful or frankly desperate, they were all looking for deals, asking prices, checking out packages: what will a new hip cost, by itself, and with bigger breasts thrown in? What about a package for two—a facelift for me, Lasik eye surgery for my companion? How much for a bridge, a root canal, ivf, angioplasty, gastric bypass surgery.... This is my budget, what can I get for it?
It might sound discordant, this price-tagging of body parts, but for Indian private hospitals, nothing is more musical than these noises from a global healthcare bazaar. They demonstrate that an idea that seemed absurd at the start of this decade has entered the realm of reality: that people from the West will travel thousands of miles, to so-called cholera country, for medical treatment—if the price is right, and the quality is right. It's an idea with big money attached to it: medical tourism is forecast to become a $2.3 billion business for India by 2012. Some analysts predict it could be the next major driver of the Indian economy after information technology—if the industry and the government play their cards right.
If 2003 and 2004 saw a trickle of refugees from the healthcare systems of western countries seeking medical treatment in India, in 2005 it became a stream, much of it fuelled by a blast of free publicity from programmes like 60 Minutes. Western TV crews accompanied often elderly people to India, filmed them hobbling out of Third World airports, with bhangra on the soundtrack, and driving into First World tertiary hospitals with the best technology money could buy. They showed them being "swamped by staff" and "feeling like kings", as one delighted patient described it, and seen by western-qualified senior consultants within an hour of arrival—which could be 2 am.
The crews tracked the pilgrims' progress, finding their way into an operating theatre where a surgeon obligingly delivered a tribute to the British system that trained him. To complete the picture, they also took gruesome shots of operations being performed at public hospitals and tell-tale ones of a row of empty beds in a poor ward at the Apollo Hospital. But the main message came through loud and clear: white people getting knees replaced, hips resurfaced, and dental work done at bargain-basement prices by experienced doctors who knew their job. British tabloids went to town on teenager Elliot Knott who successfully underwent spine surgery here last August after being told to wait a year for an operation by the National Health Service.
That the publicity was good for business shows in the numbers: British-Gujaratis Jagdish and Dipa Jethua, who saw a business opportunity in facilitating medical travel, could only send four patients to India for major surgery in January 2005. In December, however, thanks to Elliot, and other high-profile visits arranged by their start-up, Taj Medical Group, they were able to send 27. Most private hospitals saw a marked upward trend in western arrivals last year, most of them from the UK, US and Canada.
Vishal Bali, CEO of the Wockhardt Hospitals group, told Outlook that from the second half of 2004 and through 2005, the number of western patients went up to between 8 to 10 per cent, from the 1 to 2 per cent that it had been previously. The Escorts Heart Institute and Research Centre (ehirc) in Delhi said that of over 1,500 foreign patients received last year, about 700 were from non-SAARC countries, including the US, UK, CIS, and the Gulf, a significant change from previous years. Individual doctors are seeing the difference, too. Dr Mohan Thomas, a Mumbai and Goa-based cosmetic surgeon, says his practice got 1,200 international patients last year, double the number from the previous year.
The Apollo Group saw an overall five per cent increase in the number of western medical tourists, according to executive director (finance) Sunita Reddy, despite no special effort to market to them. But at Apollo's flagship Delhi hospital, which gets more medical tourists than its other hospitals, the arrivals from some countries seem to have doubled. For example, it got around 80 American patients from April to November last year, more than the entire number in the previous financial year.
Many of those mouse-clicking their way to a hospital bed in India are escapees from western medical crises: whether it's waiting lists for complicated elective surgeries in the UK and Canada, which can't deliver the free healthcare they promise; or the uninsured and under-insured in the US, where medical treatment is extortionately expensive. Any international marketing executive—and every upmarket private hospital now has one—can recite the numbers in her sleep: 8,50,000 waiting for a hospital bed in the UK, 45-million plus uninsured in the US.
Medical value-travellers, as hospitals like to call them, are also people looking for body shapes that insurance companies won't pay for and dreams that even efficient public healthcare systems won't deliver, like those of the 5 feet 4 tall Frenchman who recently came to India for a leg-lengthening operation. Many are also in quest of treatments not available at home, like hip resurfacing, less radical than hip replacement, but yet to be approved by the US Food and Drug Administration.
Carry On, Doctor
The Americans, the British, the Canadians, they are all coming. The tourist attraction: a hospital.

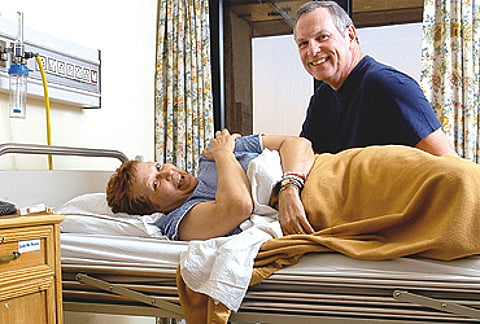
Marlene and Paul Smith; Canadian
Treatment: Spinal fusion surgery
"Much of Marlene’s pre-operative pain has gone. We’re 100 per cent satisfied. We paid $19,000, including airfare. In the US, the metal alone for her back would have cost $40,000."
EHIRC's chief surgeon Dr Naresh Trehan recently operated on an 83-year old Canadian cardiac patient who needed a valve replacement with a bypass, but had been turned down by doctors back home. "No doctor was willing to do it for him. It's my specialisation, patients with 10 or 20 per cent heart function. I told him the risk was less than five per cent," said Trehan.
Contrary to the popular stereotype, not every medical tourist is dying to see the Taj. He could be someone for whom a hospital room is the only piece of India he can handle. In a month's stay at Apollo Hospital for complicated surgery to correct his wife Marlene's curved spine, Paul Smith, from Barrie, a small picture-postcard town in Ontario, left the hospital only once, on a trip to the airport to sort out ticketing. "With Marlene in bed, why would I want to sightsee?" he said.
It was desperation that drove Paul to type "surgery in India" into a search engine after reading a story about successful treatment in India in The Barrie Examiner. Agonising pain kept his wife in bed for 16 to 20 hours a day, and the wait for an appointment with the right kind of doctor—leave alone surgery—was no less painful. Google took Smith to the Jethuas in Warwickshire and they found him spinal surgeon Dr Yash Gulati in Delhi The Smiths e-mailed him 15 questions through Taj Medical Services, covering the range from AIDS to aftercare, and booked their seats after they got his answers.
They are going home in a few hours and they won't be returning. One giant leap into the unknown was probably enough. And yet, they couldn't be more grateful, raving about their doctor, dreaming about a better life for Marlene, determined to spread the word about India.
Fortunately for the tourism ministry not all medical tourists confine themselves to hospital rooms. Amitabh Kant, the bureaucrat who helped successfully reinvent Kerala as God's own Ayurvedic paradise, is leading the ministry's initiative to promote India as a "global healthcare destination". So, after incredible temples, incredible tigers and incredible yoga, it's now going to be incredible doctors backed by incredible technology. Glossy brochures, prepared with the help of ad agency Ogilvy and Mather, feature men and women in spotless white coats bending over patients against backdrops of sleek medical hardware.

Sheryl Weidner; American
Treatment : Plastic surgery
"There is a different energy here, a different mood...a lot of nurturing. It’s much more personal than in the States," says Sheryl, a teacher from Oregon. Seen here with friend Serena Taylor who made a snap decision to buy herself an eyelift.
The patients in the brochure seem mostly white and middle-aged, for a reason: Kant is aiming way beyond the harried middle classes from SAARC countries, Afghanistan and poorer African countries who have been flocking to India for specialised medical care which their countries lack. They, too, are coming in rising numbers, especially from Afghanistan and Africa, and sure, hospitals want their custom. But for reasons of both prestige and money, what really excites both government and industry is the fatter wallets in western countries with ageing populations and rising healthcare costs—and the Gulf, where seekers are finding it harder to access medical treatment in the West, post 9/11.
It's definitely not the titled rich that are showing up here. Cosmetic surgeon Mohan Thomas's upcoming patients include a pair of London cabbies, husband and wife, coming for facelifts. But even a schoolteacher from Bognor Regis can book a nice room when a hip replacement costs less than half of what it does back home. If they like the main course, western patients will also splurge on side dishes. Like Briton Barry Peters, who came to get a hip replaced, and got his teeth done as well, paying less for the whole treatment, including airfares, than just the dental would have cost him in London. Or Serena Taylor from California, who came to look after her friend seeking plastic surgery, and decided to buy an eyelift. It must be like eyeing a pricey handbag for several weeks and suddenly finding it at 80 per cent off. What else can you say but, "I'll have that"?
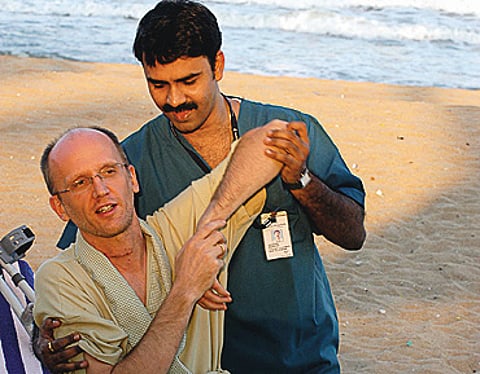
Hospitals, hotels and spas are serving up more temptations. The Apollo Group, which already offers its patients a post-op package, including the services of paramedics, at Fisherman's Cove, a beach resort outside Chennai, is tying up with the Taj group of hotels for transfers to 38 leisure hotels. "A hospital cannot replace a hotel. We should not keep these patients in hospital a minute more than required, we must send them to a place where they can recuperate," says Apollo group chairman Dr Prathap Reddy.
In Bangalore, patients can check out of leading private hospitals, and convalesce in places like Soukya, a sprawling health farm on the outskirts of the city. With an in-house team of ayurvedic physicians and allopathic doctors on call, when needed, its medical director, homeopath Dr Isaac Mathai, claims to have the "lowest doctor-patient ratio in the world". It's the detox destination for Indian software and media tycoons, and its international guests range from spiritual gurus (Deepak Chopra) to Nobel laureates (Archbishop Desmond Tutu) and Eurotrash (Sarah Ferguson). Last year they also included Ellen Parry, who runs a garage in Wales. She moved there after back surgery at the city's MS Ramaiah hospital. Back home in Wales, Ellen is still ecstatic. "Amazing!", she said on the phone from Wales when asked to describe her India experience in one word.
She is exactly the kind of medical tourist Kant wants multiplied. "Forward integration with hospitals, backward integration with holistic Indian systems of medicine," is his mantra, and it's clear why: ayurveda and the rest are products that Thailand and Singapore don't bring to the healthcare supermarket. They are uniquely ours, and already contribute significantly to India's rapidly growing tourism sector. "Integration" is a favourite word in the healthcare industry, too. If at one end of the spectrum there's Soukya, which is both spa and medical centre, and other places like it studding the lush greenery of Kerala, at the other, it's mainstream hospitals discovering "wellness" with a vengeance. Judging by the talk on the hospital circuit, it won't be long before every upmarket private hospital offers ayurvedic massages, aromatherapy, mudbaths, pranic healing, yoga, the works. And full-fledged departments of alternative medicine, with homeopaths, naturopaths, and unani medicine specialists on board to deliver that authentic dose of India.
Scot Johnson; American
Treatment: Cervical disc replacement
"I heard about medical treatment in India from the TV show 60 Minutes. Big American hospitals are full of Indian doctors, that’s how I knew they’d be good."
Top private hospitals are also vying with each other in other ways to attract an international clientele. As in an accelerated race for the latest hardware—you can't miss the giant boards advertising the latest scanner—and for that prized certificate by the Joint Commission International (JCI) in the United States, a non-governmental body that accredits international hospitals meeting exacting American standards. The early birds who have it, such as Apollo in Delhi and Wockhardt in Mumbai, display it big, and other hospitals are in the queue. "The fact that we are JCI-accredited is a symbol of quality assurance for patients in the western world. To them, quality is foremost, even over cost," declares Bali of Wockhardt.
The hospital room is changing too, with globalisation clearly the spur, though all CEOs maintain that demanding Indian patients are driving the changes, too. John Connell, a primary school teacher from Southampton in the UK, who came to Wockhardt in Mumbai earlier this month for a new minimally invasive procedure to treat a hole in his heart, had the following in his hospital room: a computer, internet, a DVD player with regional compatibility that could play British DVDs, a mini-bar, a coffee-maker, a cellphone. The hospital also offered him and wife Amanda "virtual family visits"—that is, a video of them shot in the room and uploaded for their families back home. A hospital car was made available for them to move around in the neighbourhood. John's room still managed to look like a hospital room, but at new hospitals like the Max Devki Devi Heart and Vascular Institute in Delhi, it's all blonde wood, expensive blinds, and leather sofas, the work of a British designer hired by the company to get the look right. And prices? Ashmeena Ghei, international marketing head, who is already facilitating visits by a stream of international patients, quotes them in dollars: $150 for a room, $300 for a suite.
But the 2.3 billion dollar question is: Will the stream turn into a flood? And when?
Tags